Fight, Flight, or Freeze (FFF) Responses
The brain is an interesting muscle. It can do so much and yet we don’t utilize more than ten percent of its capabilities. It is responsible for all the other muscles and functions in our body, and it is multitasking all the time (consciously and unconsciously). It has this neat thing called neuroplasticity, meaning despite any damage to some of its parts the muscle can be strengthened and experience some healing. In trauma this is evident in the fight or flight response, which has been expanded to include freeze and fawn. You can read more about these responses here, but it is important to understand the basic brain structures in this response system.
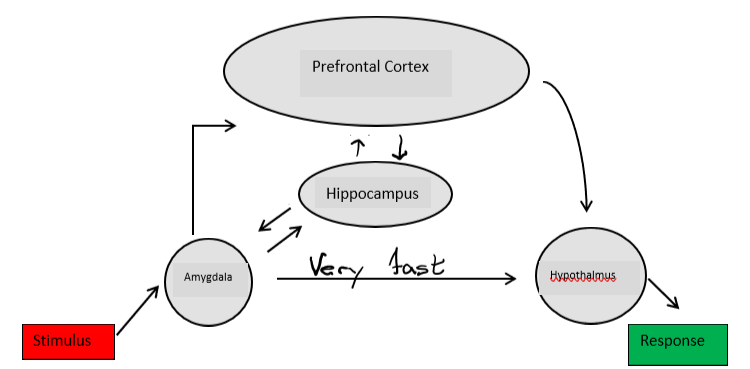
Back in the caveman days we needed to stay alive, so our bodies needed a way to keep us safe without overworking our muscles when it was not necessary. Imagine a sabretooth tiger slowly coming to the cave opening-it is crouched low to the ground, its head is lower, and ears are back, the mouth is open slightly reveling fangs and there is drool. Our amygdala senses there is a danger, checks with the hippocampus quickly (which remembers another time when it saw this scene and it was not safe), and quickly tells the hypothalamus to make the body run (flight), grab a weapon and defend itself (fight), or be really still (freeze). This all happens extremely fast, because if there was too much time to think our ancestors would have been eaten and we would not be here reading this. This is a survival response.

In order to do any of these effectively the body makes some major changes. Pupils dilate to see better, goosebumps appear on the skin as hair stands up to better sense the environment, breathing becomes quicker and shallower, and the heart rate increases-that way the muscles have more blood and oxygen to work better. Other tasks are less important and they stop, like digestion (butterflies in the stomach) and urination.
However, our body cannot remain in this heightened state for too long or it will become overworked, sometimes causing unhealthy physical effects. The prefrontal cortex is able to talk to the hippocampus and the amygdala to determine when the situation is once again safe and works to return the body to its usual functioning. In addition, if that “sabretooth tiger” was simply your neighbors’ cat walking by, the hippocampus will find it in its memory, share it with the cortex and the whole system is shut down almost immediately because there is no danger. This process is much slower than the FFF response. This all looks something like this:
How does trauma impact the FFF Response
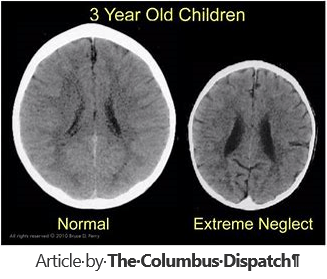
For children who have experienced complex trauma, they never know when or where the abuse may come from. Therefore, they always operate on the FFF response to a stimulus. Unfortunately they have learned that they cannot predict who or what is safe so everything starts to become a threat; they do not have the luxury to check with their memory and determine if there is something different this time that may mean they are safe. Like any muscle that we work out all the time, the FFF response becomes very strong, and the more logical thinking parts of the brain begin to atrophy. Scientists have seen images of trauma victims’ brains that show the reasoning centers of their brains are much smaller than those without trauma. At the very core they are thinking differently. They must always be ready to keep themselves safe for their own survival.
Behaviors indicative of children with complex trauma
So now we know what is happening in the brain. Many of the kids we are educating or raising are now in safe environments that no longer require the FFF response to always be on. So how can you tell when the response system is activated, even when it does not need to be?
- Trembling-increased hormones caused by the FFF response can cause muscles to shake as they are preparing for hard work
- Hyperventilating-the shallower quicker breath meant to oxygenate the blood faster
- Complaints of “chest pains” -increased heart rate pumping blood faster to the system
- Sweating-perspiration increases to keep the body from overheating during the survival response
- Hypervigilance-always scanning and watching for potential danger, always “in the ready”
- Tunnel Vision-focus on one stimulus causing distress and unable to shift focus. This could be on an object, behavior, or topic of conversation.
Providing a supportive environment/Trauma Informed Care
There are many ways to be supportive to a child who needs to learn how to manage their survival response and become better at assessing the people and situations around them. They need tools that can help delay the automatic survival response long enough to let the thinking parts of the brain exercise and grow stronger, helping them make better decisions. The great thing is, the more they work out the brain, the stronger the atrophied parts can become, and they will heal. Sensory Modulation is a great tool that helps children learn ways to retrain their survival response.
- Sight-pictures of pets/family/friends they find pleasant and safe, Defocus books where they look for patterns, Seek and find books where they have to locate specific objects
- Sound-music and sounds the child finds pleasant. This may take some adult supervision for appropriateness. Playing or resuming playing a musical instrument. A loved one’s voice pre-recorded.
- Smell (*warning: smell is the fastest way to trigger a positive or negative reaction, smell works directly on the amygdala)-favorite perfume of a loved one, favorite food, favorite dessert
- Taste-fireballs, favorite food/drink, salty things, sour things
- Vestibular rocking, swinging
- Tactile-manicures, head rubbing/scratching, soft or hard items, favorite blanket or material,

This is a basic outline and understanding of how trauma impacts the brain of a child and how we can support resiliency. It is important with any of these tools to offer choice whenever possible. This can be empowering to a child who has felt their life was completely beyond their control, including their safety. Just because you like something does not mean they have to like the same things. Help them identify what they find helpful. These can change from day to day. Once thy find these things take the time to show interest and learn about them. That way, when the brain is thinking in pure survival mode, the child can rely on you to provide those coping tools. And don’t forget the power of play. Play is where children work out their struggles and can find/practice good coping skills.
Remember, it’s not “What’s wrong with you?” but rather “What happened to you?“
Now, have a little fun and find these important words in the word search below: